
Latest News
 Boyfriend accused in slaying of Hampden sheriff’s assistant, former legislator’s top aide
Boyfriend accused in slaying of Hampden sheriff’s assistant, former legislator’s top aide
 UMass basketball: Matt Cross reportedly enters transfer portal
UMass basketball: Matt Cross reportedly enters transfer portal
 Revised plan to combat bullying in Amherst regional schools questioned
Revised plan to combat bullying in Amherst regional schools questioned
 Wheeling for Healing returns to South Deerfield to raise money for cancer treatment
Wheeling for Healing returns to South Deerfield to raise money for cancer treatment
 Sadiq to leave Amherst middle school principal role
Sadiq to leave Amherst middle school principal role
 Northampton seeks bids to redevelop former Registry of Deeds property
Northampton seeks bids to redevelop former Registry of Deeds property
 Hadley’s Brad Mish, Northampton’s Elianna Shwayder top Hampshire County finishers at 128th Boston Marathon
Hadley’s Brad Mish, Northampton’s Elianna Shwayder top Hampshire County finishers at 128th Boston Marathon
 Softball: South Hadley’s Ella Schaeffer records 500th career strikeout in loss to East Longmeadow
Softball: South Hadley’s Ella Schaeffer records 500th career strikeout in loss to East Longmeadow

Organizers ramping up for bigger Northampton Pride this year
NORTHAMPTON — Under new organizers and a nine-week planning schedule, Pride returned to the queer capital of Northampton last year after a three-year hiatus, and it’s back to stay.Hampshire Pride, the nonprofit that revived Pride in the Pioneer Valley...

Crocker School kids draw on historical picture books for library banner project
AMHERST — An unfolded brown paper bag is being transformed, through use of crayons, pencils and paint markers, into a banner showcasing an acclaimed American naturalist, artist and academic.“I think Anna Comstock was very impressive in her work,” says...
Most Read
 ‘Our hearts were shattered’: Moved by their work in Mexico soup kitchen, Northampton couple takes action
‘Our hearts were shattered’: Moved by their work in Mexico soup kitchen, Northampton couple takes action
 Springfield man charged with murder in Holyoke stabbing
Springfield man charged with murder in Holyoke stabbing
 Amherst-Pelham schools look to address school absences with new plan
Amherst-Pelham schools look to address school absences with new plan
 Two men dump milk, orange juice over themselves at Amherst convenience store
Two men dump milk, orange juice over themselves at Amherst convenience store
 Next 5-story building cleared to rise in downtown Amherst
Next 5-story building cleared to rise in downtown Amherst
 Three Amherst Regional Middle School counselors absolved of Title IX offenses
Three Amherst Regional Middle School counselors absolved of Title IX offenses
Editors Picks
 All about conviction: PVPA team wins state, heads to nationals of Mock Trial Championship
All about conviction: PVPA team wins state, heads to nationals of Mock Trial Championship
 Spring brings new art: A look at what's on tap in April at selected local galleries
Spring brings new art: A look at what's on tap in April at selected local galleries
 News Briefs: Roadwork in Plainfield; bake sale in Hadley
Three Amherst Regional Middle School counselors absolved of Title IX offenses
News Briefs: Roadwork in Plainfield; bake sale in Hadley
Three Amherst Regional Middle School counselors absolved of Title IX offenses
Sports

High school ultimate preview: Amherst, Northampton hoping for big seasons
The defending Division 1 state champions are going to look much different this spring. After capturing the state’s top ultimate Frisbee title in 2023, only six players return from that roster return to the Amherst boys team for head coach Joe...
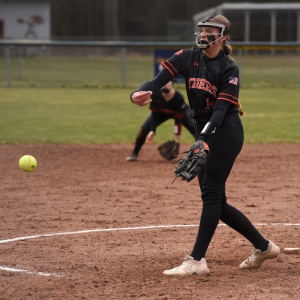
 High school: Northampton softball slugs past Mahar for season's first victory (PHOTOS)
High school: Northampton softball slugs past Mahar for season's first victory (PHOTOS) Baseball: Smith Academy can't overcome early deficit in 13-6 loss to Mahar
Baseball: Smith Academy can't overcome early deficit in 13-6 loss to Mahar High schools: Holyoke boys volleyball sweeps Athol for 5th straight victory (PHOTOS)
High schools: Holyoke boys volleyball sweeps Athol for 5th straight victory (PHOTOS) More history for Tiger Woods. He makes the Masters cut for a record 24th time in a row
More history for Tiger Woods. He makes the Masters cut for a record 24th time in a rowOpinion

Rachel Vigderman: Area women ending silence over weaponization of rape
I want to commend Sara Weinberger for her column “The appalling silence over the atrocities of October 7th” [Gazette, April 15]. As co-president of the Northampton/Amherst Chapter of Hadassah I would like to report that area residents, along with...
 Maggie Baumer: Access to prosthetics and orthotics for physical activity a right, not a privilege
Maggie Baumer: Access to prosthetics and orthotics for physical activity a right, not a privilege
 Toni Doherty: 2020s essential workers: Oxymoron?
Toni Doherty: 2020s essential workers: Oxymoron?
 Timmon Wallis: More funding for Ukraine not the answer
Timmon Wallis: More funding for Ukraine not the answer
 Columnist Razvan Sibii: How to welcome a refugee family into your community
Columnist Razvan Sibii: How to welcome a refugee family into your community

Business

Tea Guys of Whately owes $2M for breach of contract, judge rules
WHATELY — Tea Guys LLC must pay more than $2 million to a Baltimore tea company due to a breach of contract, a Franklin County Superior Court judge has ruled.The small business in Whately was sued last summer by Zest Tea LLC and had two bank accounts...
 Recognizing an ‘inspiring force’: City business owner honored with Black Excellence award
Recognizing an ‘inspiring force’: City business owner honored with Black Excellence award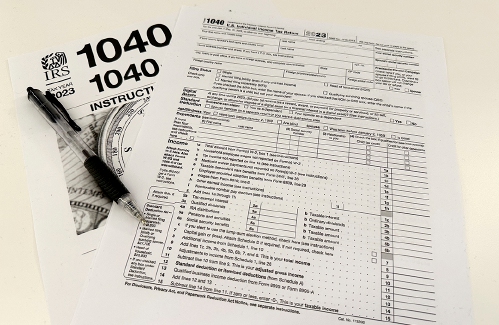 Consumer Corner with Anita Wilson: A two-day reprieve in tax filing deadline offers time for tips
Consumer Corner with Anita Wilson: A two-day reprieve in tax filing deadline offers time for tips Sublime Systems lands $87M federal award for low-carbon cement plant in Holyoke
Sublime Systems lands $87M federal award for low-carbon cement plant in Holyoke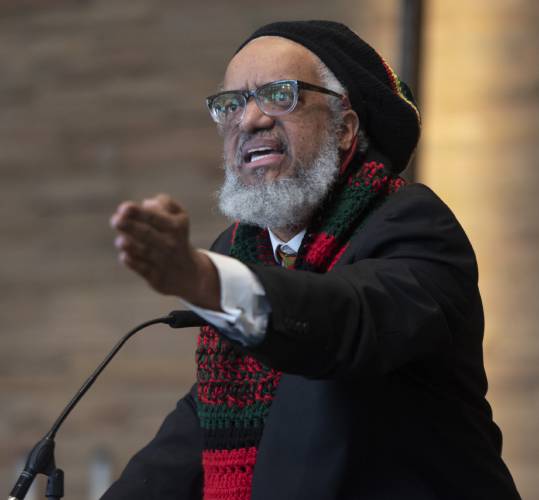 Black business group presses demand for Amherst relief funds
Black business group presses demand for Amherst relief funds
e-Edition
Arts & Life

Speaking of Nature: Indulging in eye candy: Finally, after such a long wait, it’s beginning to look like spring is here
I have just about reached the end of my patience with the winter of 2024. I realize that this may sound a bit strange, especially because we are now in the beginning of spring, but those of us who bore the brunt of the April snowstorm may sympathize...
 Weekly Food Photo Contest: This week’s winner: Nicholas Horton of Northampton
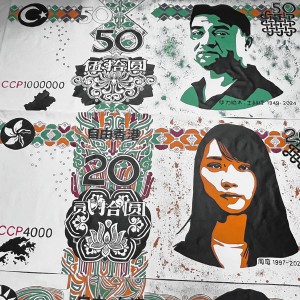
Weekly Food Photo Contest: This week’s winner: Nicholas Horton of Northampton What does freedom look like today? On view at Williams College, seven Black American artists interpret the meaning of emancipation
What does freedom look like today? On view at Williams College, seven Black American artists interpret the meaning of emancipation Book Bag: ‘Dear Oliver: An Unexpected Friendship With Oliver Sacks’ by Susan B. Barry; ‘Benjy’s Messy Room’ by Barbara Diamond Goldin
Book Bag: ‘Dear Oliver: An Unexpected Friendship With Oliver Sacks’ by Susan B. Barry; ‘Benjy’s Messy Room’ by Barbara Diamond Goldin Only Human with Joan Axelrod-Contrada: To journal or not to journal: Advice for when journaling feels like it’s holding you back
Only Human with Joan Axelrod-Contrada: To journal or not to journal: Advice for when journaling feels like it’s holding you backObituaries
 Virginia Seney
Virginia Seney
LEEDS, MA - Friendly Ice Cream Corporation announces the slashing of their coffee ice cream production after the passing of Virginia Ann Heon Seney on April 13, 2024 at the age of 89. Born ... remainder of obit for Virginia Seney
 Elizabeth A. O'Brien-Means
Elizabeth A. O'Brien-Means
Williamsburg, MA - Elizabeth Ann O'Brien-Means, 71, of Briar Hill Rd. passed peacefully on Thursday at the Senior Living Campus at Linda Manor in Leeds. Betsy, as family and friends called ... remainder of obit for Elizabeth A. O'Brien-Means
 Kathleen A. Dunn
Kathleen A. Dunn
Northampton, MA - Kathleen Ann (Spellman) Dunn, 79, of Northampton, MA, passed away on April 8, 2024 surrounded by family, at Community Hospice House in Merrimack, NH. She was born in P... remainder of obit for Kathleen A. Dunn
 Joseph Walter Walas Jr.
Joseph Walter Walas Jr.
Joseph Walter Walas, Jr. East Haddam, CT - Joseph Walter Walas, Jr., 73, of East Haddam, formerly of Durham, and husband of the late Linda (Good) Walas, passed away on Wednesday, March 27, 2... remainder of obit for Joseph Walter Walas Jr.

